


Case report:
Patient with advanced bile ducts cancer, with recurrence in bile ducts prothesis, was qualified for palliative PDR brachytherapy. The aim of treatment was opening a passage in bile ducts and prevention of jaundice. Percutaneous trans-hepatic technique allowed the passage of a catheter through the stricture. A transhepatic cholangiogram was initially performed under fluoroscopic control. After the site of obstruction was identified, a flexible catheter was inserted into the biliary tree to an appropriate depth, under fluoroscopic control. To avoid the catheter changing procedure, we used a 10 French catheter, which could also be used as a conduit to place the brachytherapy catheter, thus facilitating the procedure for both team and patient. Treatment planning was based on radiography taken with the applicator in place and the cholangiogram showing the malignant stenosis in prothesis. The radio-opaque wire had markers at intervals which indicated the placement of the radioactive source. An X-ray unit, the IBU (Integrated Brachytherapy Unit), was used for 3D planning. Radiation dose was prescribed at 10mm from the source axis. PLATO brachytherapy planning system was used. Target Volume encompassed prothesis visualized at cholangiography and a 1 or 2cm margin taken proximally and distally. PDR - BT was given in one fractions of 20 Gy (25 pulses of 0.8 Gy/hourly.
Case gallery:
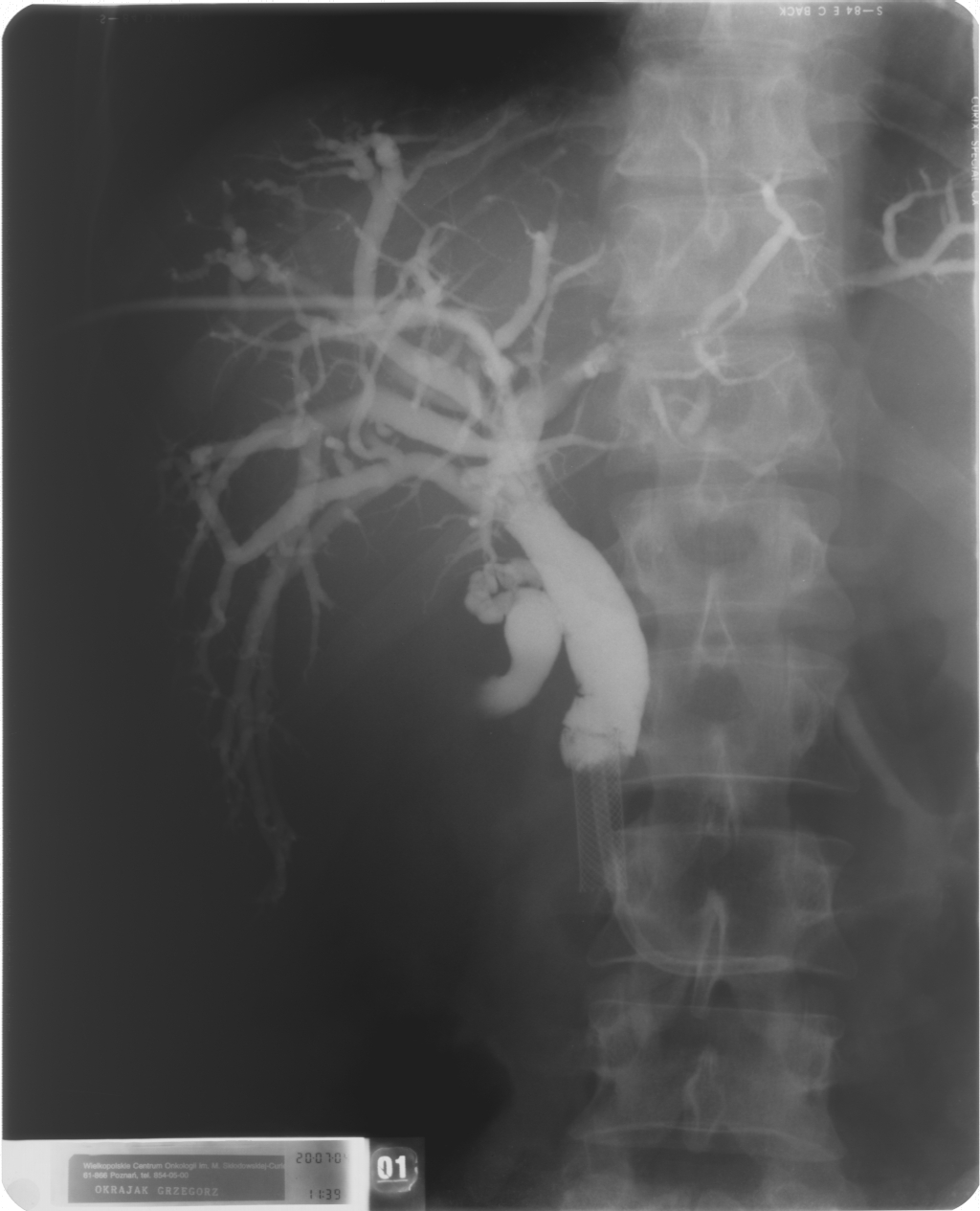
Cholangiography - bile ducts visualised with contrast, before application of brachytherapy catheter (French 5), 10 F catheter inserted using transhepatic technique, prothesis

Cholangiography - bile ducts visualised with contrast, after application of brachytherapy catheter (French 5), 10 F catheter inserted using transhepatic technique, prothesis